Transoral thyroidectomy with vestibular approach: a new technique in Colombia
<p>Recently, a transoral endoscopic thyroidectomy viavestibular approach (TOETVA) was performed in Colombia, preserving the most relevant anatomic elements and co the basic principles of surgery, including safety, adequate approach, avoiding bleeding and contamination during the procedure. The procedure had a duration of 210 minutes, had no peri or early postoperative complications, and patient was discharged home the same day of the procedure. Patient was reevaluated on postoperative day 3, with no hematoma, good cervical function and no post-operative complications. Pathology revealed follicular adenoma.</p>
Introduction
Transoral endoscopic surgery was first described as an experimental approach in 2008 by Witzel et al [1]. Later, Anuwong used this technique in humans and published the first cohort of patients in 2015 [2]. TOETVA is a minimally invasive technique, and was developed as one of the natural orifice transluminal endoscopy surgery (NOTES).This approaches offers a clear advantage in cosmetic results, with a clear advantage over the classic procedures described by Kocher many years ago. However, higher rates of conversion to open surgery and surrounding tissue damage were reported initially but subsequently decreased over time [3, 4]. In this case report, we describe the first procedure of this type performed in Colombia.
Case Report
A 50-year-old female consulted was referred due to a solitary thyroid nodule located in the right thyroid lobule. The nodule measured 12x11x9mm, oval shaped with well-defined borders, heterogenous with a solid area of 2mm, small micro calcifications were present and with no extrinsic vascular supply. FNA was performed, reporting Bethesda IV, follicular neoplasia. After discussing and explaining to patient new surgical approach, patient provided informed consent and patient was scheduled to undergo TOETVA.
Surgical Technique
First phase of surgery: after nasal end tracheal intubation and general anesthesia, patient’s neck is exposed using interscapular and cervical supports with head immobilization; the surgical equipment was set up as described in Figure 1. Surgical asepsis using iodine based product eye protection was performed.
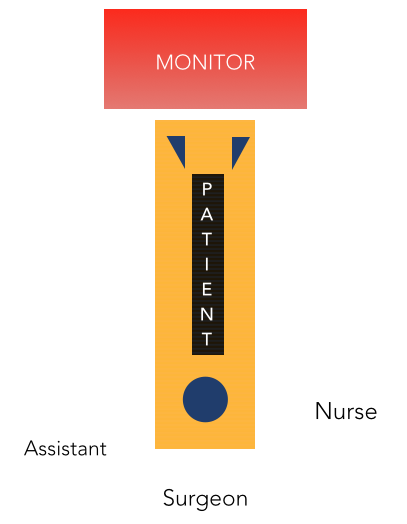
Figure 1: disposition of team and equipment in the operating room. Second phase: the oral cavity was cleaned using a solution with chlorhexidine 0.05%. A after locating the central region of the oral cavity and the vestibular region, a 10- mm incision was performed and extended up to the mandible symphysis. Using Veres needle, subplastimal hydro dissection with approximately 20cc was performed in 3 axes (central, right and left). Caution to not surpassthe sternocleidomastoid muscle and avoid the great vessels was exerted. After blunt dissection of the subplastimal plane, a 10mm central trocar and 2 additional 5 mm trocar were placed at the level of the inferior molars, in order to prevent injury of the mental nerve, according to the technique described by Dr. Anuwong (Figure 3). Later, insufflations to 5-6 mmHg with CO2 and aperture of the planes were performed until reaching and fixating the parathyroid muscles.


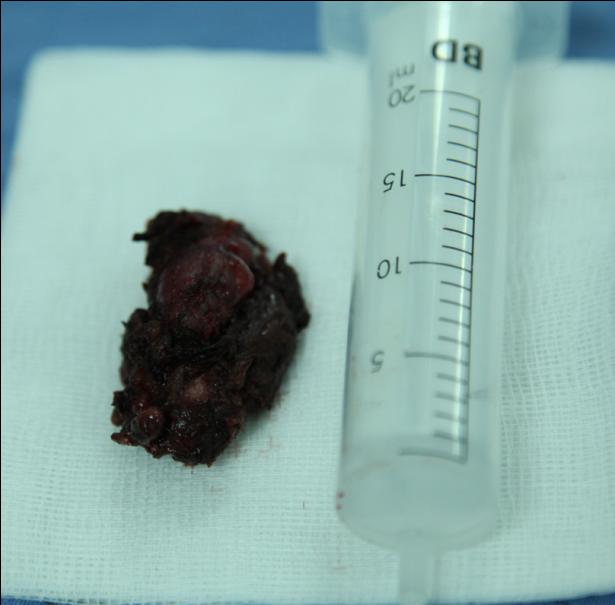
After ensuring a safe approach, an incision in the isthmus was made using last generation energy, and dissection of superior thyroid artery and vein with preservation of superior parathyroid glands was performed. Later, blunt dissection through the tracheoesophageal groove until identification of recurrent laryngeal nerve. The same procedure was repeated with the right lower thyroid lobule until exeresis and extraction of surgical piece (Figure 4). Intraoperative pathology reported 11x10x9mm follicular adenoma, which was later confirmed in definitive pathology, and surgical procedure was concluded. Patient was discharged home 7 hours after the procedure was concluded uneventfully (Figure 5).

Discussion
The evolution of thyroid surgery has not changed significantly until 20 years. The development of minimally invasive endoscopic techniques, initially implemented in abdominal and base of cranium surgery, showed satisfactory results after learning curves for the procedure were achieved by the surgeons. Based on this experience, novel approaches and techniques have been developed that compete with conventional procedures. Along with these new techniques, new devices and energies to achieve hemostasis have been developed, allowing safer interventions [5]. Endoscopic surgery, and it’s implicit evolution, improve peri and postoperative quality of life, lead to a shorter and with less complication hospital stay and provide a better cosmetic result as compared to traditional approaches [6, 7, 8, 9, 10, 11, 12, 13]. With our experience, as head and neck surgeons with endoscopic training, do not underestimate the limitation of this technique, described before by Diogni et al [14], and include patient’s with undifferentiated cancer, thyroid cancer with high risk of relapse, nodal stage N1b, constant loss of CO2 insufflations, giant goiter, collision of instruments, prior radiotherapy and thyroiditis. The surgical time was 210 minutes, with an approximate bleeding of 5 ml. The patient was discharged 7 hours after concluding the procedures, with no complications in the following days and in constant communications with the surgical team. Patient was reassessed after 3 days, with no functional disturbances found in patient’s neck and in good overall condition. Despite being a technique, which we consider, will be the future of thyroid surgical resection. In Colombia it is not implemented as the standard technique because of the cost that this represents for the health system (15- 20% more than conventional thyroidectomy). However, cost- effectiveness analysis has not been carried out between the two techniques in Colombia.
Conclusion
Transoral endoscopic thyroidectomy via vestibular approach appears to be a safe and reproducible technique, with a positive impact in quality of life. Given the described limitations of this technique, we believe this approach represent a new alternative as long as patient is selected appropriately.
The authors do not have any conflict of interest to disclose.
References
-
Witzel K, von Rahden BH, Kaminski C, Stein HJ (2008) Transoral access for endoscopic thyroid resection. Surg Endosc 22(8): 1871-1875
-
Anuwong A (2016) Transoral Endoscopic Thyroidectomy Vestibular Approach: A Series of the First 60 Human Cases World J Surg 40: 491-497.
-
Rattner D, Kalloo A, ASGE/SAGES Working Group (2006) ASGE/SAGES working group on natural orifice translumenal endoscopic surgery. Surg Endosc 20(2): 329-333.
-
Clark MP, Qayed ES, Kooby DA, Maithel SK, Field F. Willingham FF (2012) Natural orifice translumenal endoscopic surgery in humans: a review. Minim Invasive Surg 12: 189296
-
Dralle H (2006) Impact of modern technologies on quality of thyroid surgery. Langenbecks Arch Surg 391(1): 1-3.
-
Miccoli P, Berti P, Materazzi G, Minuto M, Barellini L (2004) Minimally invasive video-assisted thyroidectomy: five years of experience. J Am Coll Surg 199(2): 243-248.
-
Tan CT, Cheah WK, Delbridge L (2008) ‘‘Scarless’’ (in the Neck) endoscopic thyroidectomy (SET): an evidence-based review of published techniques. World J Surg 32(7): 1349-1357.
-
Yeung GH (2002) Endoscopic thyroid surgery today: a diversity of surgical strategies. Thyroid 12(8): 703- 706.
-
Duh QY (2003) Presidential Address: minimally invasive endo- crine surgery–standard of treatment or hype? Surgery 134(6): 849-857.
-
Henry JF (2008) Minimally invasive thyroid and parathyroid surgery is not a question of length of the incision. Langenbecks Arch Surg 393(5): 621-626.
-
Ng JWT (2004) Minimally invasive surgery or minimal-incision thyroidectomy? Arch Surg 139(7): 802.
-
Cunningham SC (2006) Minimally accurate nomenclature. Surg Endosc 20(6): 998
-
Cuschieri A (1992) ‘‘A rose by any other name...’’ Minimal access or minimally invasive surgery? Surg Endosc 6(5): 214
-
Dionigi G, Tufano RP, Russell J, Kim HY, Piantanida E, et al (2017) Transoral thyroidectomy: advantages and limitations. J Endocrinological Invest.
- Shaping Healthy Futures: Pediatric Endocrine Breakthroughs of 2025
- Precision Medicine in Obesity: Customizing Treatment for 2025
- The Thyroid Revolution: How 2025 is Redefining Hormone Health
- Editorial- Targeting Immunometabolism for Generating Innovative Therapies for Cancer
- Current Knowledge of Chickenpox
- Correlation of Preinjection Values of Gonadotropins and Estradiol Level with Clinical and Radiologic Evidence of Sufficient Pubertal Suppression in Girls with Central Precocious Puberty